by Laura Landro at the Wall Street Journal
A new push is under way to improve the care people get after they call 911, when minutes can make the difference between life and death. The inside of the ambulance is changing as it is being stocked with new techniques and devices to improve trauma victims’ survival. Laura Landro has details on Lunch Break.
One Problem: Medical advances that save lives in hospitals and on the battlefields are often slow to become available to civilian emergency responders.
There is plenty of room for improvement: Survival rates among sudden-cardiac-arrest patients, for example, vary widely among different regions in the country. One problem: Medical advances that save lives in hospitals and on the battlefields are often slow to become available to civilian emergency responders.
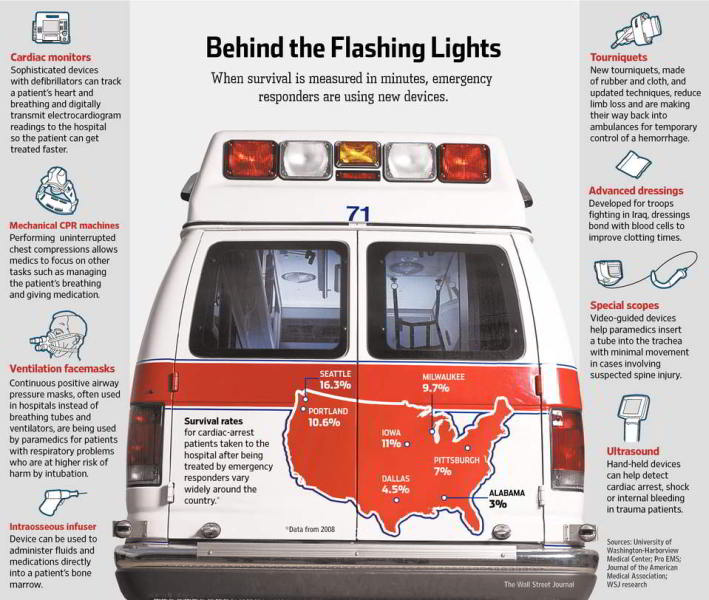
Emergency medical systems and ambulance companies are driving the efforts to change. A growing number of communities are training their 911 call centers to instruct bystanders by telephone in the best way to administer cardiopulmonary resuscitation, or CPR, which has been shown to increase a patient’s chance of surviving. Some emergency responders are equipping ambulances with new technologies like digital transmission systems to beam electrocardiograms to hospitals and quick-clotting bandages, developed for troops fighting in Iraq, to stop bleeding faster. Paramedics—the most skilled providers of pre-hospital emergency care—also are being trained to chill cardiac-arrest patients after resuscitating them, as is often done in hospitals; the procedure has been shown to increase patients’ chances of surviving without brain damage.
Cardiac arrest kills close to 300,000 people a year in the U.S., and trauma is the No. 1 killer of people under age 44. Of those who die, more than half do so in the first two hours, before they ever arrive at a hospital.
“The goal is to train the paramedics to be as good as physicians when treating patients in the field,” says Andreas Grabinsky, head of emergency and trauma anesthesia at the University of Washington-Harborview Medical Center in Seattle, where the city and county EMS providers offer free training programs to other emergency systems.
 It is difficult to introduce innovations. Emergency medical systems are generally overseen by a state or regional agency and vary by community. Ambulances may be operated by fire departments, hospitals, volunteer groups or private companies. When a 911 call comes in, firefighters, who at minimum have basic emergency medical technician certification and may also be paramedics, are dispatched as first responders. Ambulances staffed by paramedics with advanced life support equipment are summoned either by their proximity to the call or on a rotation.
It is difficult to introduce innovations. Emergency medical systems are generally overseen by a state or regional agency and vary by community. Ambulances may be operated by fire departments, hospitals, volunteer groups or private companies. When a 911 call comes in, firefighters, who at minimum have basic emergency medical technician certification and may also be paramedics, are dispatched as first responders. Ambulances staffed by paramedics with advanced life support equipment are summoned either by their proximity to the call or on a rotation.
The goal is to train the paramedics to be as good as physicians when treating patients in the field. Andreas Grabinsky
Emergency responders must meet basic regulatory standards, but it is generally voluntary whether they equip their vehicles with the latest technologies and train their crews in the most up-to-date procedures and skills. A 2008 study led by Graham Nichol, director of the University of Washington-Harborview Center for Prehospital Emergency Care, found that survival rates for EMS-treated cardiac arrest in 10 major regions varied from a high of 16.3% in Seattle to a low of 3% in Alabama. New data for 2010, though not yet available by city, show the national average has been improving, according to Dr. Nichol.
Some ambulances are being fitted with machines that provide continuous chest compressions so paramedics can insert breathing tubes and perform other lifesaving procedures without pausing to restore breathing.
Another new device finding its way into some ambulances is a digital transmission system that speeds sophisticated electrocardiogram readings to the hospital so cardiac patients can get treated faster. When heart-attack victims require a balloon angioplasty, a procedure that opens blocked blood vessels, hospital staff often rush to get this done within 90 minutes, the time required to avoid heart-muscle damage. The transmission device is usually combined with a monitor to track the patient’s pulse, heart signs and breathing.
The new digital technology helped save the life of 43-year-old Robert Douglas, who passed out at his home in Cambridge, Mass., in August, feeling weak with chest pains radiating to his left arm. Paramedics from the Cambridge fire department and ambulance company Professional Ambulance and Oxygen Service Inc., known as Pro EMS, performed the ECG at Mr. Douglas’s home. Trained to interpret electrocardiograms, they transmitted to Mount Auburn Hospital images showing signs of a type of heart attack in which an artery is totally blocked by a blood clot. Doctors in the ER were able to get Mr. Douglas in for a balloon angioplasty within 42 minutes.
 Pro EMS, a Cambridge, Mass., ambulance company, train to use hand-held ultrasound devices, which can assess
Pro EMS, a Cambridge, Mass., ambulance company, train to use hand-held ultrasound devices, which can assess
internal bleeding.
“Before this system, the communication was like a child’s game of telephone,” with paramedics and doctors at the hospital often not understanding each other’s verbal descriptions, says Todd Thomsen, an emergency physician at Mount Auburn. “Had this system not been in place or had there been other delays, Mr. Douglas would have had a worse outcome.” Mr. Douglas says he has recovered fully.
Pro EMS has been participating in a program at Emory University in Atlanta called the Cardiac Arrest Registry to Enhance Survival, or CARES, which the ambulance company says has helped it double its cardiac-arrest-survival rate in the last two years. CARES has been gathering data from 911 call centers, EMS providers and hospitals around the country since 2004 to compare results and to help communities improve emergency care.
At Pro EMS, which submits data to the CARES program as part of Cambridge’s fire-department EMS system, staff members undergo about five times the national standard of 72 hours of continuing education, refresher courses and recertification in CPR and advanced life-support skills, says chief executive Bill Mergendahl. The company has also purchased 16 sophisticated monitors, including the ECG systems, cardiac- and breathing-monitoring devices and defibrillators at a cost of $25,000 each. “It can get expensive to add new technologies to EMS, but we are improving outcomes that lead to savings in health care all the way down the line,” Mr. Mergendahl says.
 Shown are paramedics undergoing
Shown are paramedics undergoing
training to listen to lung sounds.
The San Francisco fire department, which began participating in CARES in 2009, trained all 1,400 of its staff last year in updated CPR and advanced cardiac-life-support techniques. The department purchased electronic monitors that provide visual feedback about the effectiveness of chest compressions, and it is using new airway tubes that are easier to insert without interrupting CPR.
Fire department captain Justin Schorr says the emergency survival rate in the city has risen over the two-year period. But the city wanted also to measure survival in another way—-for victims whose cardiac arrest was witnessed and someone, either a bystander or EMS staff, intervened with CPR or a defibrillator. “We focused on how well we did when we had the best chance to help someone,” he says, and results improved dramatically—from 9% to 23% over the period.
Researchers also are investigating possible new techniques to boost survival rates. For example, people admitted to the hospital ER at high risk for traumatic brain injury or hemorrhagic shock currently are given a dose of estrogen within two hours of injury, which has been shown to reduce dangerous inflammation. The Resuscitation Outcomes Consortium, a group of 10 regional centers based at the University of Washington that conducts clinical trials, plans to investigate whether estrogen given intravenously before the patient gets to the hospital would improve survival.
View original article: View Original WSJ Article